Dr. Deepak Chhabra, Dr. K Mrityunjay
Morton’s toe (or Morton’s foot, Greek foot, “Royal toe“, “LaMay toe“, “Sheppard’s toe“, Morton’s syndrome, long toe) is the condition of a shortened first metatarsal in relation to the second metatarsal. It is a type of hypoplastic metatarsal or Brachymetatarsia (where there is one or more shortened metatarsal)

This is how Morton’s foot looks like
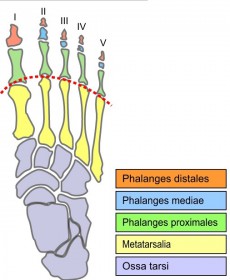
The correct term for Morton’s Toe is Morton’s Foot Syndrome, named after Dr. Dudley Morton who was a foot doctor of some fame back in the 1930’s. Morton’s toe is a little misleading, because this condition isn’t really a long toe, meaning the phalanges (toe bones). It is the relative length of the Metatarsal foot bones, specifically the relative lengthdifference between the first and second that defines this foot shape. For most feet, a smooth curve can be traced through the joints at the bases of the toes. But in Morton’s foot, the line has to bend more sharply to go through the base of the big toe, as shown in the diagram.
You don’t need an x-ray to determine if you have Morton’s Toe. If the space between your first and second toe appears to be deeper, not wider, but deeper than the space between your second and third toes, you have Morton’s Toe which is also sometimes just called Morton’s Foot.

The lines depict the misalignment of metatarsals
Etiology, Symptoms and Pathomechanics:
Although commonly described as a disorder, it is sufficiently common to be considered a normal variant of foot shape (its prevalence varies with different populations). Many people with Morton’s toe have no problems from it.
The most common symptom experienced due to Morton’s toe is callusing and/or discomfort of the ball of the foot at the base of the second toe (Metatarsalgia). The first metatarsal head would normally bear the majority of a person’s body weight during the propulsive phases of gait, but because the second metatarsal head is farthest forward, the force is transferred there. Pain may also be felt in the arch of the foot, at the ankleward end of the first and second metatarsals. In shoe-wearing cultures, Morton’s toe can be problematic. For instance, wearing shoes with a profile that does not accommodate a longer second toe may cause nail problems such as the curving of the nail.
Janet G. Travell, MD, coauthor of The Trigger Point Manual, concluded that Morton’s toe was “a major perpetrator of musculoskeletal dysfunction and pain.” While the prevalence of Morton’s toe is around 10% in the general population, among people suffering from musculoskeletal pain and seeking medical help, it is thought to be well over 80%. The reason Morton’s toe is often a precursor to musculoskeletal pain is its association with excessive pronation of the foot. When weight bearing, the longitudinal arch of the foot drops, and the ankle rolls inward.
This excessive pronation causes two major postural and functional problems:
- The leg is functionally shortened or lengthened.
- The leg is rotated internally.
Just one functionally shortened toe behaves just like a structural short leg, unbalancing the pelvis by dropping one hip lower. This can cause various degrees of scoliosis(improper lateral curves of the spine). The internally rotated leg causes a forward rotation of the pelvis, typically more on the side where the foot hyperpronates the most. The forward rotation of the hips causes changes in the kyphotic (anterior/posterior) curves of the spine and in general causes a forward-leaning, head-forward posture. The compromised posture combined with the torques created by internal leg rotation is often the cause of both joint and muscle pain ranging from knee and hip pain to low and general back pain and shoulder and neck pain. It is also believed by some to be associated with headaches and TMJ dysfunction, although this is not universally accepted.
Diagramatic representation of morton’s toe
This foot structure is known to cause and perpetuate musculoskeletal problems. Problems start with the feet and the list is long.
Foot Pain
- Metatarsalgia (ball-of-foot pain)
- Morton’s Neuroma
- Metatarsal Stress Fractures
- Plantar Fasciitis
- Calluses
- Bunion
- Hammer, Claw and Mallet toes
Lower Extremity Pain
- Ankle Pain – Weak Ankles
- Shin splints
- Tight, Sore and Tired Calf Muscles
- Knee pain
- Tight IT Bands
- Runner’s Knee (Chondromalacia)
- Fractured Meniscus
- ACL Tears
- Sciatica Pain
- Arthritis
Back and Neck
- Scoliosis & Kyphosis
- SI Joint Pain
- Sciatica (Piriformis Syndrome)
- Low-Back Pain
- Upper Back and Shoulder Pain
- Neck Pain (head forward posture)
Dr. Dudley Morton also observed that people who had Morton’s Toe experienced profound changes in their gait. He noticed many people rotated their feet outward. He observed postural changes. His solution to the problem was to make what he later patented, called a Morton’s extension. It was a rigid plate placed under the inside of the foot that extended beyond the length of the first metatarsal to approximately the same length as the second metatarsal. In addition Dr. Morton thought the first Metatarsal was hypermobile, but what he missed was that the first metatarsal was also elevated, so that when a person tried to walk with their legs and feet in proper alignment, the first metatarsals and the big toes were not properly weight bearing.
As has later been established, the Elevated First Metatarsal affects many more people than does Morton’s Toe. About 80% of the population has an elevated first metatarsal. Although accurate statistics are hard to find it is estimated that 20-30% of the population has Morton’s Toe.
Treatment:
Some doctors might propose surgery to make the first and second metatarsal more equal in length. What Dr. Morton considered a hypermobile first metatarsal often manifested in a splayed first metatarsal that pointed away from the foot. Changing the metatarsal length would not affect its orientation, and problems like bunions would still be a likely result.
As it turns out, the correction for an elevated first metatarsal also greatly improves the mechanics of the Morton’s Toe foot. This correction consists of a small pad placed underneath the head of the first metatarsal – thickness up to 1/4 inch. This approach was suggested by Dr. Morton himself as well as Dr. Janet Travell who wrote the recognized text books on myofascial pain. She considered correcting the Morton’s Foot problem essential to treating muscle pain.
Conclusion:
This Article gives us an insight for patients with postural syndrome and Myofascial pain. It suggests that checking out for existence of morton’s toe and its secondary biomechanical effects is important in such patients & it can be an important finding in patients with musculoskeletal ailments which tend to recur despite best of treatment.
Refrences:
Morton, D. J. “Metatarsus atavicus: the identification of a distinct type of foot disorder”, The Journal of Bone and Joint Surgery, Boston, 1927, 9: 531-544.
Schimizzi, A; Brage, M (September 2004). “Brachymetatarsia”. Foot Ankle Clin 9 (3): 555–70,
http://en.wikipedia.org/wiki/Morton’s_toe#cite_note-Review04-1
aka. Morton’s Foot aka. Morton’s Foot SyndromefckLRaka. Greek Foot http://www.mortonstoe.com/
Janet G. Travell, David G. Simons (1997). Myofascial Pain And Dysfunction – The Trigger Point Manual (The Lower Extremities). Volume 2. Lippincott Williams & Wilkins